Minoxidil for Hair Loss: Myths, Truths, and Practical Use
4 min read
By Lookmax Analyzer Team — Last updated
Sep 4, 2025Minoxidil is the most accessible, evidence-based over-the-counter option for pattern hair loss. But the internet is a mess of claims. Let’s separate what’s real from what’s noise.
TL;DR: For male/female pattern hair loss, topical minoxidil (2–5%) is FDA-approved and can slow loss + regrow some hair if used consistently for months. Low-dose oral minoxidil (LDOM) is prescription/off-label—promising for some, but not superior to topical in at least one head-to-head RCT at 24 weeks. Expect possible temporary shedding early on; results plateau by 12–18 months and reverse if you stop.
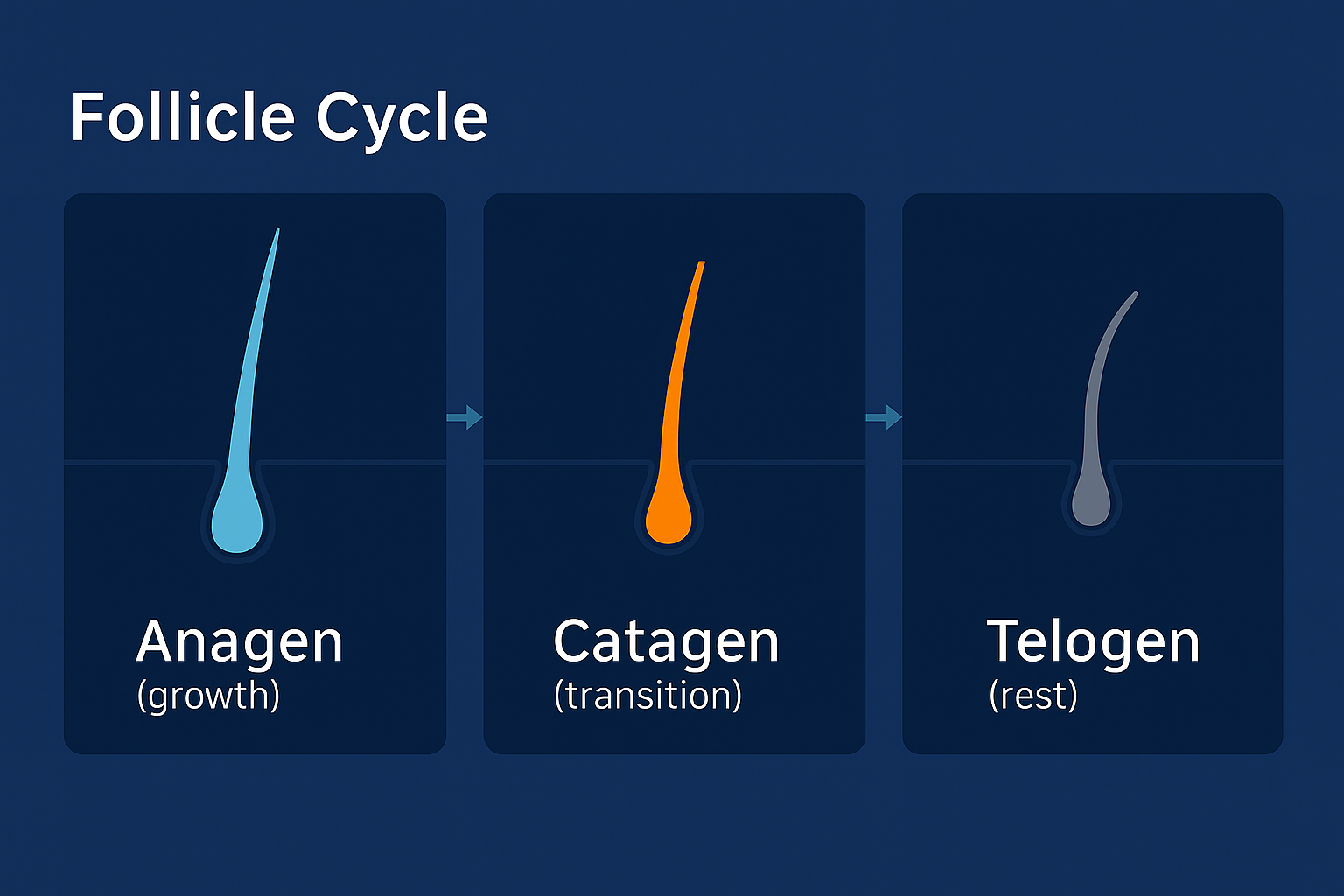
The follicle cycle moves through growth (anagen), transition (catagen), and rest (telogen). Treatments like minoxidil promote more follicles to enter the growth phase, improving density and coverage.
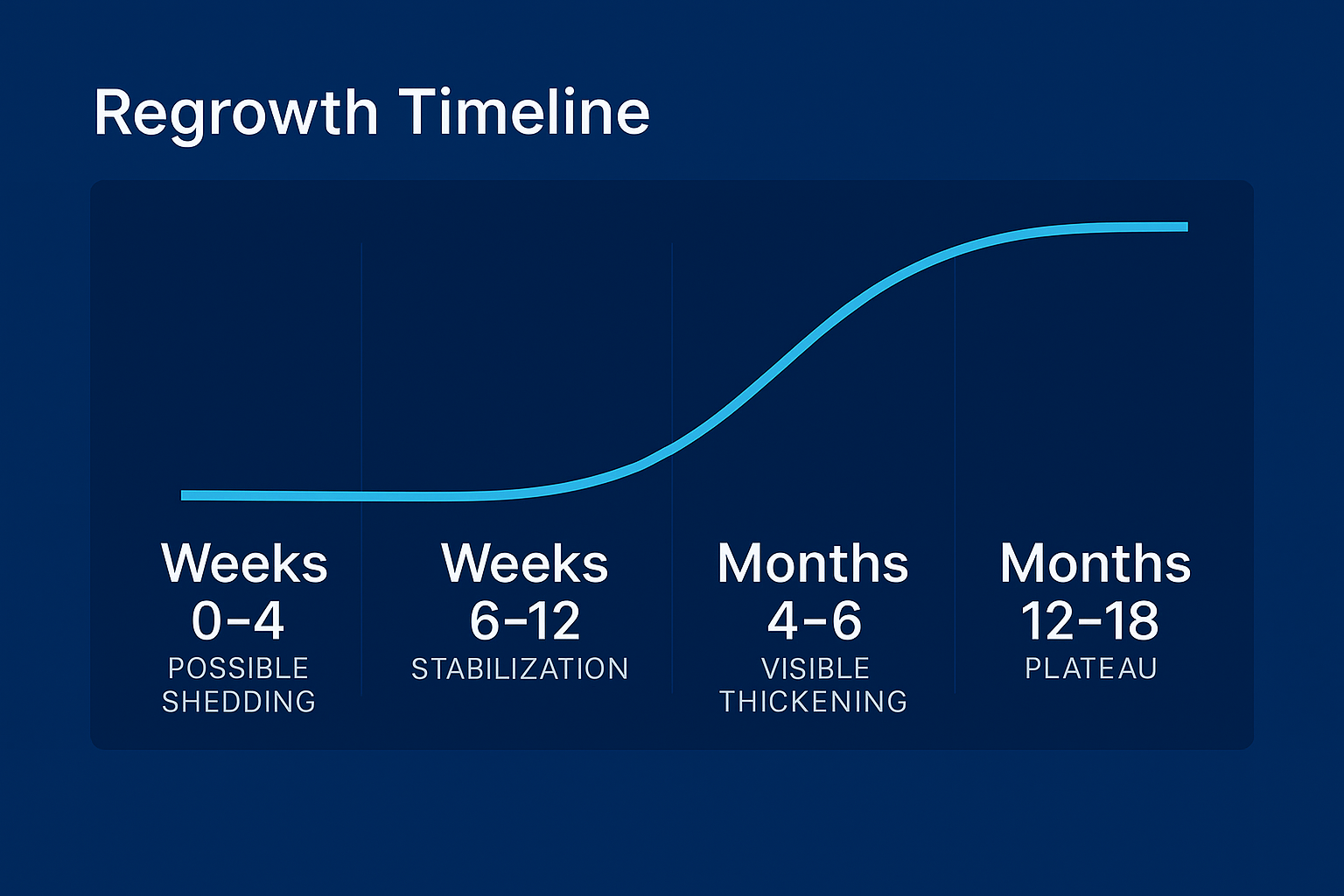
Typical response curve: early shedding can occur, then stabilization and gradual thickening. Results often plateau around 12–18 months with continued use.
What minoxidil actually does#
- Extends anagen (growth) phase and can increase hair diameter and density—best evidence at the vertex and frontal scalp.
- Topical 2–5% is FDA-approved for androgenetic alopecia (AGA) in men and women (foam or solution; 5% foam once daily is common for women, 5% twice daily for men; some regimens vary).
- Low-dose oral minoxidil (LDOM) (typically 0.25–5 mg/day) is off-label; growing evidence supports efficacy, but a 24-week RCT was not superior to topical 5% twice daily in men. Discuss risks with a clinician.
Myths vs. truths#
Myth: “Minoxidil stops baldness permanently.”
Truth: It works while you use it; benefits fade if you stop. Response varies—some slow further loss and regrow modestly; others mainly stabilize.Myth: “5% is the same as 2%.” Truth: 5% outperforms 2% in RCTs (faster, more regrowth). Choose foam vs. solution based on scalp sensitivity/feel.
Myth: “If I shed at the start, it means it’s making things worse.” Truth: Early shedding (2–6 weeks) can happen as follicles switch into growth; it’s typically temporary (often settles by ~3–12 weeks).
Myth: “Oral minoxidil is always better.” Truth: LDOM is convenient and helps some patients, but was not superior to topical in a 24-week male RCT (5 mg oral vs. 5% topical BID). It also has systemic side-effects risks (edema, tachycardia, hypertrichosis), so it’s prescription + monitoring.
Myth: “It only works on the crown.” Truth: Evidence shows benefit at vertex and frontal regions, though individual response varies.
Myth: “Women can’t use 5%.”
Truth: Women’s 5% foam is FDA-approved (once daily is common); discuss with a dermatologist if irritation or facial hair growth occurs.
How to use it (simple, realistic plan)#
Topical (most users)
Where: Apply to dry scalp, not the hair shafts.
How much: Solution ~1 mL per application; foam ~ half capful (check label).
- When:
Men: often 5% twice daily (some do once daily 5% foam; consistency > perfection).
Women: 5% foam once daily or 2% twice daily, per label/advice.
Timeline: Tiny changes by 3–4 months, clearer gains by 6–12 months; max around 12–18 months. Keep going to maintain.
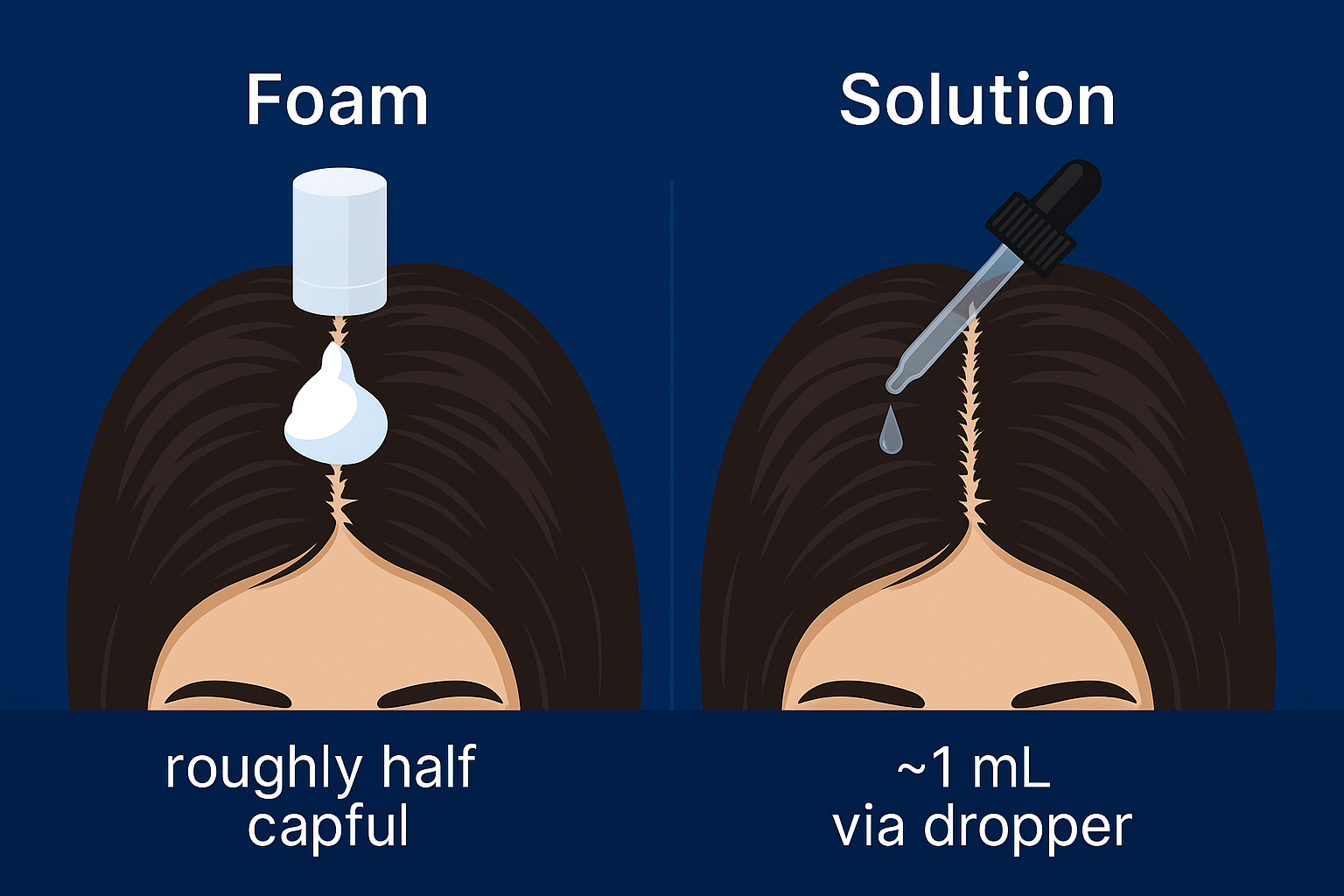
Apply to the scalp (part hair in lines). Foam: roughly half capful. Solution: ~1 mL via dropper. Let dry before styling or sleep.
Oral (LDOM; off-label—doctor only)
- Consider if topical is impractical/irritating or for diffuse patterns—but discuss risks (BP changes, edema, palpitations, unwanted body hair). Start low, monitor.
Shedding playbook: Early shedding is common. Stay the course 8–12 weeks unless you have concerning side effects. Some dermatologists overlap topical while starting oral to blunt the “dread shed” (clinic-dependent).
Combos & boosters (evidence snapshot)#
Minoxidil + microneedling can improve outcomes vs. minoxidil alone in some studies—seek trained guidance for technique/frequency.
Finasteride (men) targets DHT; combo with minoxidil often outperforms either alone (finasteride is Rx in many regions, discuss risks).
Lifestyle: Address iron, thyroid, severe caloric deficits, and stressors with a clinician if suspected contributors.
Side effects & safety#
Topical: scalp irritation, itching, dandruff-like flaking; occasionally facial hypertrichosis from runoff. Lowering frequency, switching foam↔solution, or applying at night can help.
Oral (LDOM): hypertrichosis, ankle edema, tachycardia; rare serious effects—requires medical supervision (especially if cardiac or BP history).
When to stop/seek care: persistent chest pain, rapid heartbeat, dizziness/syncope, sudden swelling—stop and contact a clinician.
Who benefits most#
Earlier, milder AGA generally responds better.
Consistent daily use beats on-off patterns.
Realistic goal: stabilization + visible thickening in miniaturized areas—not teenage density.
Recommended products#

Kirkland Minoxidil 5% Foam (6-month supply)

Rogaine 5% Minoxidil Solution (Men)

Rogaine 5% Foam (Women’s Once Daily)
Want tailored, non-medical tips?#
Sources & further reading#
Olsen, E. A., et al. (2002). 5% vs 2% topical minoxidil in AGA — 5% superior at 48 weeks. J Am Acad Dermatol.
Penha, M. A., et al. (2024). Oral 5 mg vs topical 5% BID — no superiority of oral at 24 weeks (men). JAMA Dermatol.
Suchonwanit, P., et al. (2019). Meta-analysis: 5% minoxidil demonstrates significant density increase versus 2% and placebo. PMC Review.
JAAD Int. (2024). Combating “dread shed”: The impact of overlapping topical and oral minoxidil on temporary hair shedding during oral minoxidil initiation. 15:220–224.